by Inventeur, LLC.
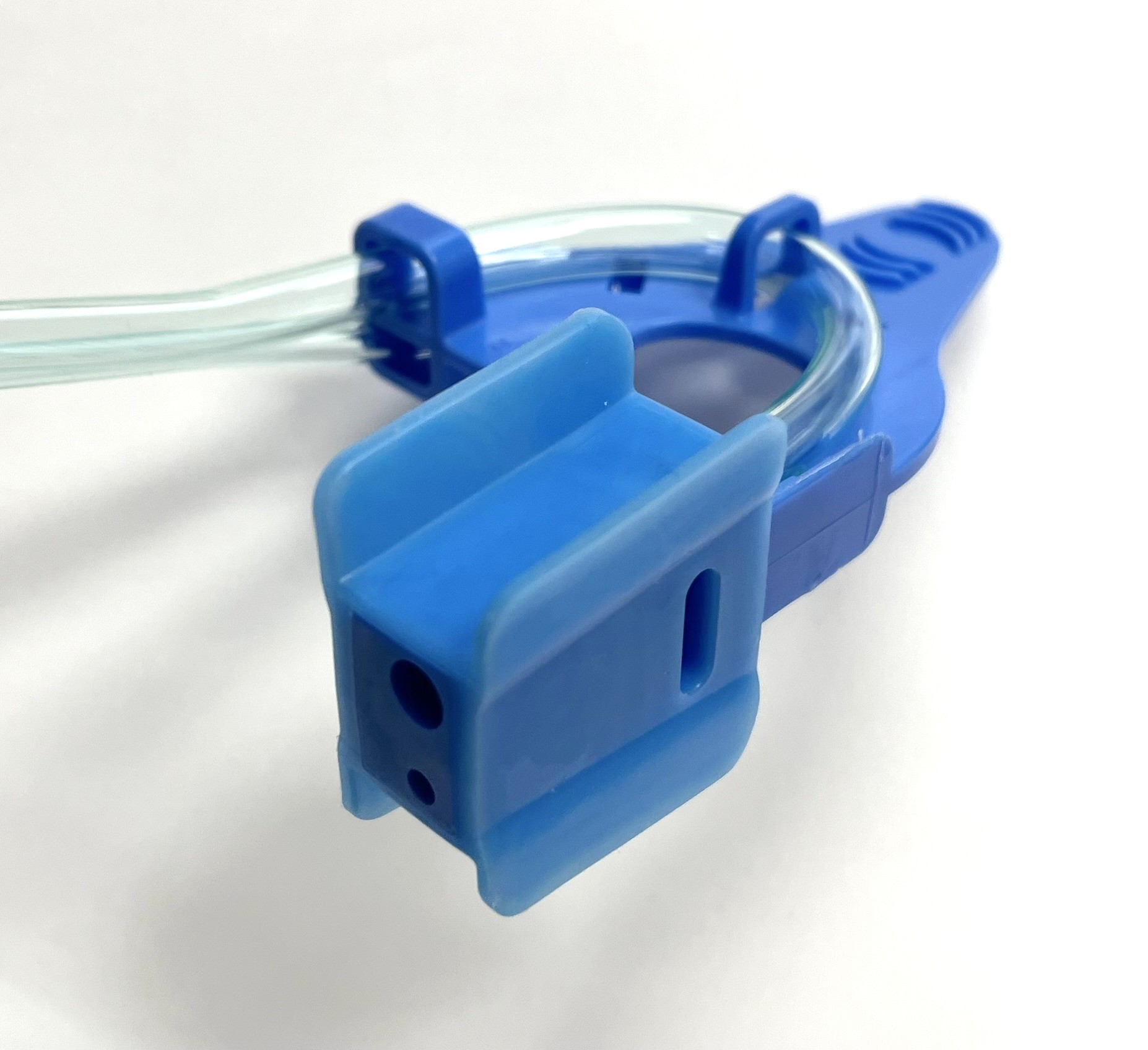
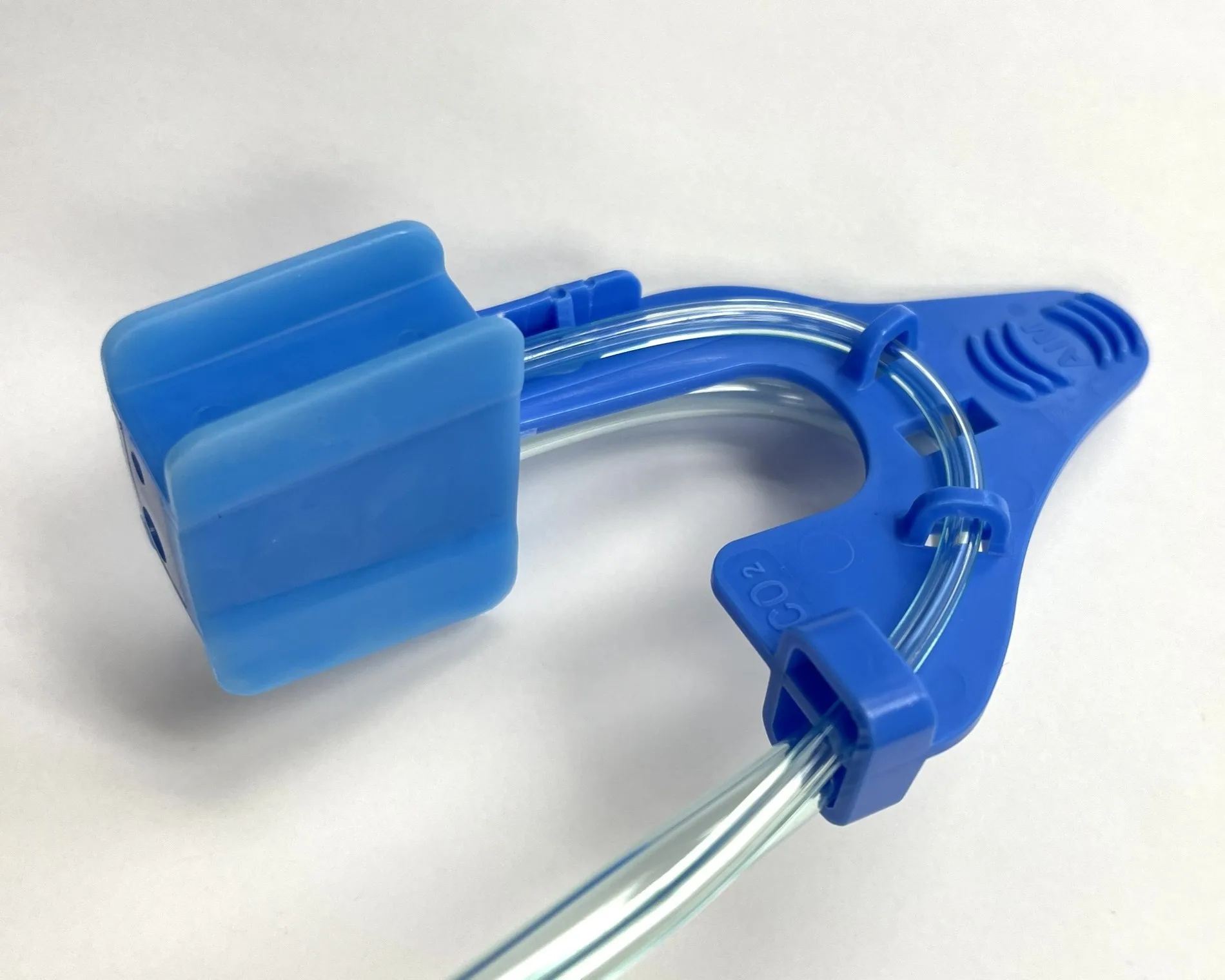
The AIM bite block integrates oxygenation, capnography, and airway rescue into one optimized sedation device.
Non-operating room anesthesia (NORA) is the fastest-growing segment in anesthesia,[1] but oxygen delivery and patient monitoring haven't kept pace with the increasingly complex procedures and higher-risk patients.
FiO2 20–40%. Unreliable capnography in patients converting to oral breathing.
FiO2 30–60%. Delayed oral airway placement during endoscopy. Upward displacement may increase the risk of ocular injury during sedation, when eyes are typically untaped.
Expensive, cumbersome, and extremely high oxygen consumption. At around 3 cents/L and 60 L/min flow, a 30-min case costs $54 in oxygen alone.
A single intraoral device that delivers direct pharyngeal oxygenation with integrated CO2 sampling from pre-sedation through recovery.




With oxygen delivery comparable to the high-flow cannula, but at a fraction of the cost and without the cumbersome setup, AIM is ideal for the NORA setting.
M. Zales, MD
I recently used AIM on a morbidly obese patient undergoing endoscopy. Despite the challenging body habitus, oxygen saturation stayed 100% throughout the procedure. The reliability in this high-risk setting was impressive and clinically reassuring.
M. Blevins, CAA
AIM gives me the confidence to perform high-risk sedation procedures.
B. DeBoard, CRNA
What impressed me the most about AIM was the speed in correcting oxygen saturation after apnea. Pharyngeal oxygenation really works. This device could be a game-changer.
Todd Little, CRNA
With unobtrusive access to the oral cavity, scope placement was easier. AIM prevented hypoxic episodes without any procedural interruptions.
K. Byju, MD, Gastroenterologist
510(k) Cleared
AIM is an FDA-cleared Class II medical device. Designed, developed, and manufactured in the United States.
With continuous EtCO2 monitoring, AIM meets the ASA sedation guidelines
As procedural complexity and patient acuity increase, AIM occupies the sweet spot: higher performance than nasal cannula, lower cost than HFNC, more versatile than face mask.
| AIM | HFNC | Nasal Cannula | Face Mask | |
|---|---|---|---|---|
| FiO2 Delivered | >96% at 12LPM[2] | 100% at 70LPM | 20–40% | 30–60% |
| Continuous EtCO2 | Yes | Unreliable | Unreliable (oral breathing) | Yes |
| Immediate Oral Access | Yes | No | No | Blocked |
| Integrated Bite Block | Yes | No | No | No |
| Setup Time | <1 min | ~5 min | <1 min | <1 min |
| MRI Safe | Yes | No | Yes | Yes |
| ASA Guideline Compliance | Full | Partial | Yes | Yes |
| O2 Equipment Required | Standard | Specialized | Standard | Standard |
| Fire Risk | Low | High | Medium | Medium |
| Staff Training | Minimal | Moderate | Minimal | Minimal |
| Space Requirements | Minimal | Significant | Minimal | Minimal |
| Maintenance | None (disposable) | Regular servicing | None | None |
| Patient Comfort | High | Moderate | High | Low |
| Cost per Procedure | $$$ | $$$$$ | $$ | $$ |
Attach the oxygen supply line and CO2 sampling line to your existing equipment.
Insert the AIM bite block intraorally, just like a standard bite block.
Deliver oxygen and monitor capnography throughout the procedure with unobstructed airway access.
NORA case volume is growing faster than any other procedural category. Every minute of airway-related interruption carries a real cost in time, disposables, and throughput. AIM is designed to reduce all three.
Continuous oropharyngeal oxygen delivery reduces desaturation events that force procedural pauses.[3] Integrated capnography eliminates separate monitoring setup. Fewer device exchanges mean fewer workflow disruptions.
AIM integrates the functions of a bite block, supplemental oxygen delivery system, and capnography sampling interface into a single disposable. Fewer SKUs to order, stock, and manage.
When per-case airway setup and management time decreases -- even by minutes -- the cumulative effect across a full procedural day enables tighter scheduling and improved room utilization.
Published data estimates OR time costs at $45-60 per minute.[4] NORA suite costs vary by facility but follow similar economic drivers. Consider your own numbers:
| Cases per week | How many NORA cases does your facility perform weekly? |
| Minutes saved per case | If AIM eliminates even 2-3 minutes of interruption or setup time, what is the weekly total? |
| Disposables replaced | How many separate items (bite block, nasal cannula, capnography adapter) does AIM consolidate? |
| Cost per disposable set | What is your current per-case spend on those individual components? |
We encourage you to run these numbers for your facility. For a detailed analysis tailored to your case volume, contact our team.
Common questions from clinicians and facilities evaluating AIM.
With advances in minimally invasive techniques, surgeries are transitioning from general anesthesia to sedation. The complex non-OR Anesthesia (NORA) procedures require higher FiO2 to prevent hypoxic interruptions. AIM's unique pharyngeal oxygenation delivers 96% and higher FiO2 near the tracheal inlet, far exceeding traditional devices.
Even though conventional devices use 100% oxygen, exhaled air in the oral cavity and sinuses dilutes oxygen delivery. AIM's pharyngeal oxygenation bypasses the mouth and sinuses. A study at the Baylor University Medical Center confirms pharyngeal oxygenation is superior to high-flow nasal cannulas. (https://pubmed.ncbi.nlm.nih.gov/38174013/).
This approach works for low-risk patients. However, oral airways are poorly tolerated by awake patients. Sedating a high-risk patient without optimal pre-oxygenation risks preventable desaturation. Additionally, an oral airway cannot be used in the recovery room for patients requiring supplemental oxygenation. AIM is non-gag inducing and can be used from pre-oxygenation all the way through the recovery room.
More questions? View the full FAQ or contact our team.
Built by anesthesiologists and engineers with deep experience in clinical practice and medical device development.
Inventor & Founder, Inventeur LLC
Practicing Anesthesiologist

Professor of Anesthesiology

Neurosurgeon

CEO, Inventeur LLC

Engineer
President & CEO, Baymar Solutions

Engineer, Product Manager
VP of Engineering, Baymar Solutions
Request a sample, schedule a demo, or ask us anything.
Or email us directly at info@macmodule.com
AIM is available through the following authorized distribution partners.

